Comparison of equivalent doses of pain medications
An equianalgesic chart is a conversion chart that lists equivalent doses of analgesics (drugs used to relieve pain). Equianalgesic charts are used for calculation of an equivalent dose (a dose which would offer an equal amount of analgesia) between different analgesics.[1] Tables of this general type are also available for NSAIDs, benzodiazepines, depressants, stimulants, anticholinergics and others.
Format
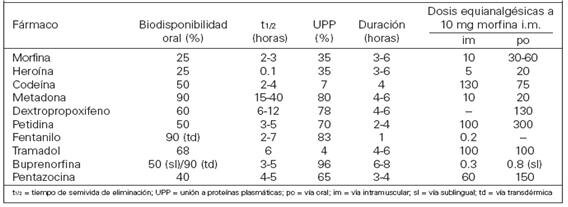
Equianalgesic tables are available in different formats, such as pocket-sized cards for ease of reference.[1] A frequently-seen format has the drug names in the left column, the route of administration in the center columns and any notes in the right column.[2][3]
Purpose
There are several reasons for switching a patient to a different pain medication. These include practical considerations such as lower cost or unavailability of a drug at the patient's preferred pharmacy, or medical reasons such as lack of effectiveness of the current drug or to minimize adverse effects. Some patients request to be switched to a different narcotic due to stigma associated with a particular drug (e.g. a patient refusing methadone due to its association with opioidaddiction treatment).[4] Equianalgesic charts are also used when calculating an equivalent dosage of the same drug, but with a different route of administration.[citation needed]
Precautions
An equianalgesic chart can be a useful tool, but the user must take care to correct for all relevant variables such as route of administration, cross tolerance, half-life and the bioavailability of a drug.[5] For example, the narcotic levorphanol is 4–8 times stronger than morphine, but also has a much longer half-life. Simply switching the patient from 40 mg of morphine to 10 mg of levorphanol would be dangerous due to dose accumulation, and hence frequency of administration should also be taken into account.
There are other concerns about equianalgesic charts. Many charts derive their data from studies conducted on opioid-naive patients. Patients with chronic (rather than acute) pain may respond to analgesia differently. Repeated administration of a medication is also different from single dosing, as many drugs have active metabolites that can build up in the body.[6] Patient variables such as sex, age, and organ function may also influence the effect of the drug on the system. These variables are rarely included in equianalgesic charts.[7][3][8]
Opioid equivalency table
This section appears to contradict the equianalgesic table in the article on oxycodone. Please discuss at the talk page and do not remove this message until the contradictions are resolved.(September 2023)
This chart measures pain relief versus mass of medication. Not all medications have a fixed relationship on this scale. Methadone is different from most opioids because its potency can vary depending on how long it is taken. Acute use (1–3 days) yields a potency about 1.5× stronger than that of morphine and chronic use (7 days+) yields a potency about 2.5 to 5× that of morphine. Similarly, the effect of tramadol increases after consecutive dosing due to the accumulation of its active metabolite and an increase of the oral bioavailability in chronic use.[citation needed]
PO: oral • IV: intravenous injection • IM: intramuscular injection • SC: subcutaneous injection • SL: sublingual • TD: transdermal "Strength" is defined as analgesic potency relative to oral morphine. Tolerance, sensitization, cross-tolerance, metabolism, and hyperalgesia may be complex factors in some individuals. Interactions with other drugs, food and drink, and other factors may increase or decrease the effect of certain analgesics and alter their half-life. Because some listed analgesics are prodrugs or have active metabolites, individual variation in liver enzymes (e.g., CYP2D6 enzyme) may result in significantly altered effects.
See also
Oripavine – for more on the comparative strength of oripavine derivatives
^"ULTRAM® (tramadol hydrochloride) Tablets Full Prescribing Information"(PDF). US Food and Drug Administration. Ortho-McNeil Pharmaceutical, Inc. March 2008. p. 4. Retrieved December 28, 2016. The mean terminal plasma elimination half-lives of racemic tramadol and racemic M1 are 6.3 ± 1.4 and 7.4 ± 1.4 hours, respectively. The plasma elimination half-life of racemic tramadol increased from approximately six hours to seven hours upon multiple dosing.
^ abcdSawynok J (January 1986). "The therapeutic use of heroin: a review of the pharmacological literature". Canadian Journal of Physiology and Pharmacology. 64 (1): 1–6. doi:10.1139/y86-001. PMID2420426.
^ abMendelson J, Upton RA, Everhart ET, Jacob P 3rd, Jones RT (1997). "Bioavailability of sublingual buprenorphine". Journal of Clinical Pharmacology. 37 (1): 31–7. doi:10.1177/009127009703700106. PMID 9048270
^ abEriksen J, Jensen NH, Kamp-Jensen M, Bjarnø H, Friis P, Brewster D (1989). "The systemic availability of buprenorphine administered by nasal spray". J. Pharm. Pharmacol. 41 (11): 803–5. doi:10.1111/j.2042-7158.1989.tb06374.x
{kind=link}